Who Owns Your OB/GYN?
Through layers of loopholes, private equity has exerted a hidden reach into Texas women’s healthcare

When a woman selects an OB/GYN, they’re selecting a doctor to guide them through some of the most intimate aspects of their medical healthcare. One might consider the doctor's gender, personality, medical specialty, and insurance affiliations. Yet rarely does one select a healthcare provider based on profit margins.
Private equity firms—financial groups that acquire businesses, restructure them, and sell them for a profit—search for OB/GYN offices as investments with entirely different criteria. Women’s healthcare is fragmented, meaning that many small independent offices make up the market rather than a single, dominant entity. Practices that lack the scale or negotiating power to resist acquisition are easy for PE firms to buy cheaply, consolidate quickly, and profit from critical women’s healthcare. In Texas, it is illegal for corporations to directly own medical practices: the Corporate Practice of Medicine doctrine forbids it to protect patients from healthcare decisions that prioritize profit over the doctor’s professional opinion. However, through layers of loopholes, the practice occurs at scale anyway.
At the height of COVID-19, patients delayed a wide variety of healthcare services in the name of quarantine. As a result, private practices were cheap to buy; private equity began purchasing OB/GYN clinics in Texas by the dozen. According to corporate filings reviewed by the Texas Signal, Unified Women’s Healthcare—whose Florida-based parent company is currently under investigation for overbilling patients—consolidated 45 previously independent OB/GYN offices under one corporate roof in a 72-hour window in May of 2020.
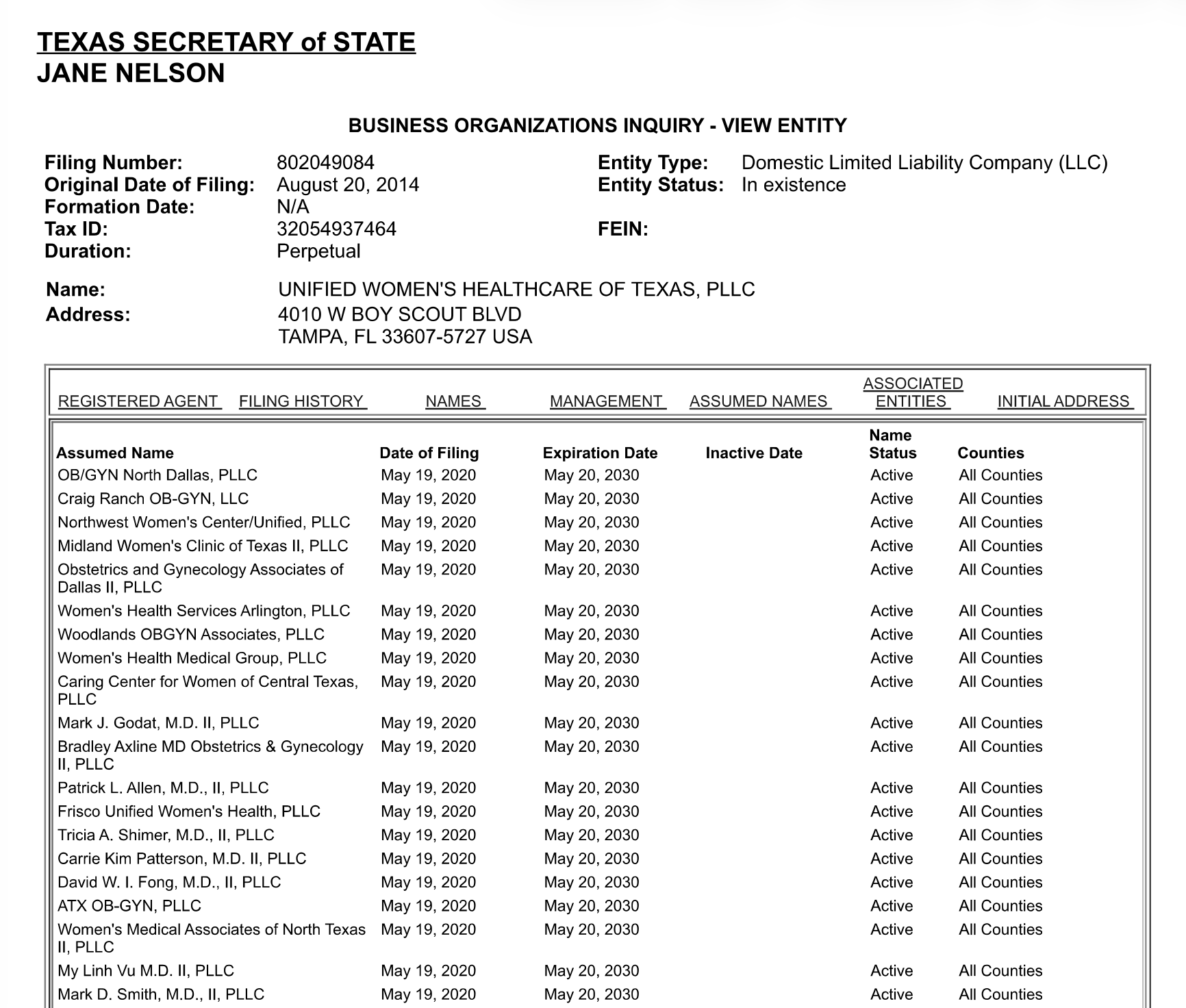

Six years later, those acquisitions have built a corporate footprint that stretches across the state. Federal Medicare records, last updated in May of 2026, show that 257 individual obstetricians, gynecologists, and certified nurse midwives now route their Medicare billing through Unified Women’s Healthcare of Texas. A separate corporation owned by a different private equity firm—OB Hospitalist Group, backed by Gryphon Investors—counts another 952 reassigned providers in the same federal database. Together, more than 1,200 professionals who deliver Texas women’s babies, perform surgeries, and manage reproductive care now send their Medicare bills through private-equity-controlled corporations.
Research shows that when PE firms control the business side of OB/GYN care, the incentives that shape clinical decisions shift. PE firms are designed to generate rapid returns for investors, not to provide long‑term community healthcare. For women in Texas, this can mean higher patient bills, shorter appointment times, reduced staffing, and the elimination of “unprofitable” services like postpartum care.
Texas’ corporate practice of medicine (CPOM) doctrine is more than a hundred years old. It stemmed from concerns dating back to the early days of American medicine: the businesses that bought and sold railroads and factories to build the country would eventually buy and sell doctors—and therefore provide treatments based on what’s profitable rather than medically productive. To this day, the CPOM holds that only licensed physicians can own medical practices—not corporations.
Yet, every state in the US with a similar rule has watched PE firms build the same four-layer workaround. First, a state-licensed doctor forms a PLCC—a professional limited liability company that the doctor owns. Then, the doctor signs a contract with a separately owned company called a Management Services Organization. Matt Parr, communications director for the Private Equity Stakeholder Project (PESP) told the Texas Signal:
“In some healthcare sectors, especially where corporate ownership rules are restricted, private equity firms use MSOs to control administrative operations, staffing, billing, contracting, and finances while physicians technically retain ownership of the clinical practice itself. That allows firms to consolidate and manage large networks of providers while maintaining layers of separation between the private equity owner and the local practice. These structures can also help limit liability.” The doctor's name stays on the door, and in exchange, healthcare providers hand over the headaches of business administration and collect a salary instead.
In the third layer, the MSO is owned by a holding company—which is often owned by another holding company, and another, and another, until ownership traces back to a PE fund. The fourth and final layer involves a DBA, or Doing-Business-As name.
“In practice, that can create a complicated web of LLCs, DBAs, management entities, and affiliated companies that may not be obvious to patients or even regulators,” said Parr. “A provider may still appear to operate under its longstanding local name even after being absorbed into a much larger private equity-backed system.”
Patients walking into their OB/GYN office see the name of a local clinic. They have no easy way to trace that brand up through the MSO contract, the holding companies, and the fund; the only way to do so involves in-depth knowledge and records requests, which often require payment, in several different states. Texas has no law requiring healthcare practices to disclose who collects the profit—the bills proposed to do so have been shot down twice.
PESP reports that in 2025, Massachusetts, California, and Oregon moved to require disclosure of private equity ownership of medical practices. Texas considered the same step in two separate bills: House Bill 4408 and Senate Bill 1595, both filed in the 89th Texas Legislature, which would have required medical practices to report changes in their ownership and control to state regulators. Patients would, for the first time, have a formal way of learning that their doctor’s practice had been absorbed into a corporate network. Both bills died in committee, after both the Texas Hospital Association and the Texas Medical Association testified against them, citing concerns about the bill’s penalty structure and “intrusive reporting requirements.”
In Texas, a woman can spend months choosing the right OB/GYN. Yet she cannot see a crucial factor: whether the practice she enters is still run by physicians or by a financial firm in another state seeking the highest profit margins. More than 1,200 Texas OB/GYNs and affiliated providers now bill Medicare through private-equity-controlled companies. At the same time, lawmakers have twice declined to require those companies to disclose who ultimately owns them. In a state that once built the Corporate Practice of Medicine doctrine to keep commerce out of the exam room, private equity has found a way in anyway.



Comments ()